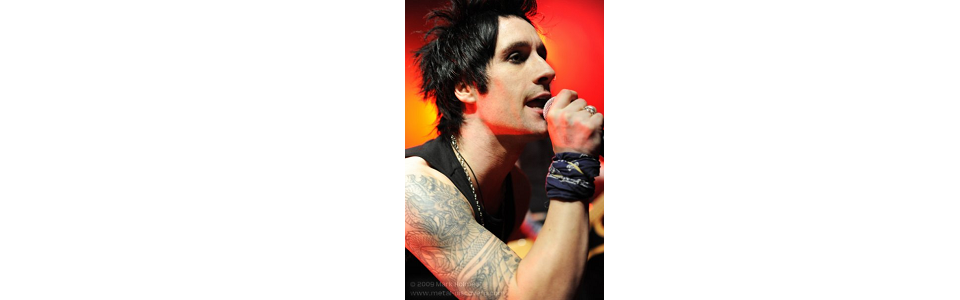
The Glitterati emerged onto the UK music scene in 2005 with their self-titled album and singles chart success. Characterised by energetic live shows, the early days were filled with the joys every young band dreams of, from recording with a legendary producer to being signed to one of the world’s biggest labels and touring America, but industry politics brought an untimely end to the band. We caught up with the former singer, Paul Gautrey, to discuss the past and the future.
Let’s start with the Glitterati if you don’t mind. That band felt unique in its honesty, both in the songs you released and in the way you spoke candidly in interviews and on stage. Members of that band said publicly that they weren’t too into modern music and that there wasn’t much decent guitar-based rock hitting the airwaves, at least in the UK. That resonated with me because I felt the same way, with bands like the Killers and Kings of Leon not filling the void. Is that still something you feel or do you think the scene has changed in the past few years? And did the Glitterati deliberately set out to try to change that and bring some excitement back into music?
We were always ourselves in interviews and onstage, sometimes we probably said too much but it made good entertainment. We didn’t set out to fill a void for anyone but ourselves, because like you said there wasn’t really much great rock music around, there weren’t any bands breaking through we loved. It seemed that people treated rock music like some ironic joke, in London especially; all hip kids throwing air guitar and rock horns became cool, [but] we probably benefitted from this too as we got signed for a shitload of money and were all over magazines like the NME, but we never wanted any part of that.
I first heard of the band on the New Kings of Rock N Roll show that aired in the late hours. You were featured on that before your debut album was released, can you tell us how that came about?
Yeah, it was a week of gigs that were broadcast on channel 4 [and] it was supposed to feature all the bands who were getting touted by the press and radio as the best new bands, some were already big and some were up and coming like us. The show we actually played was us supporting The Vines but when it went out on channel 4 they showed us and Jet, I’m not sure why, maybe because we had the same label as Jet, but I kind of wanted to show us with The Vines. I really liked them at the time but they were pretty shambolic live the night we played with them so I thought it would make us look better, ha ha!
Can you talk a bit about the early days after you moved to London and started to get noticed; did success feel to you as rapid as it appeared to the public? You’ve said previously that when you didn’t have a manager you were courted by the labels and getting free meals out of them. Did that require any effort on your part or did it just happen from your reputation as a live band?
It was rapid from the time we all moved to London as we were getting offers from all over the place within a few months, but me, John and Bill had been in bands in Leeds together for a few years before the Glitterati, Nic had already had one record deal in another band, we really were just like “Fuck it, we aren’t getting anywhere in Leeds so let’s move to london where the streets are paved with gold.” I’ve no idea what we would have done if it hadn’t happened, and luckily it happened quickly as we probably couldn’t have afforded to stay for more than a few months, we were living on one pound a day each for food.
How did you live on a pound a day?
It wasn’t a rule, we didn’t give anyone a hard time if they splashed out £2 on a burger and chips, but we were broke and had to be careful as we didn’t want to be on the next Megabus back to Leeds within a few weeks. We also had the regular nights at the posh restaurants courtesy of the labels and managers, besides Costcutter noodles were only about 15p a pack……..we ate a lot of Costcutter noodles, ha ha!
We didnt have a reputation as a live band as we hadnt played even a single gig together, we just had a demo we did at Nic’s house with our mate, we only gave it to one person – Paul Harris – who at the time worked for B-unique records and he played it to someone else, they played it to someone else and it snowballed. We were meeting all these massive labels and managers within weeks, we would bring them all to where we rehearsed and play them 3 or 4 songs live but we hadn’t played a gig together. We didn’t plan anything but everything fell into place like a dream, we signed to Universal Publishing not long after and they helped set us up with even more managers and labels, we did an indie single on Alan McGee’s Poptones label, he wanted to sign us but we ended up going with Atlantic who won us over with nights at Stringfellows and a record deal worth stupid amounts of money. We were pretty wealthy for a while, but that soon changed once we started doing things like paying £35,000 to do one album launch gig and other daft things, but we definitely had fun.
You recorded the debut album in LA with Mike Clink and I understand that there was talk of the band relocating there. Is there any truth to that and what made you choose to stay in the UK?
Yes we considered moving there, this was between the first and the second album, we weren’t on Atlantic anymore and were looking for a new label. We had just toured over there off our own backs and we were getting quite a lot of interest and people were loving us,especially in LA.
Whilst out there we signed a management deal with a big company and it looked like it was all going to happen for us like it did here; it was almost identical to when we moved to London, kind of like we were in the right place at the right time.
I wanted us to just pack up and move, things were obviously better for us there than here, some of us wanted to go but other guys just didn’t want to.
It was never spoken about at the time, the reasons for not going were usually to do with money, visas etc, but by this time the guys had their own houses and were in long-term relationships, things they didn’t want to or couldn’t just give up. I can understand that now, but I really think if we had moved at that point we would have done really well out there. Looking back, two guys left the band not long after so i can understand why they didn’t want to up sticks and move to LA if they were thinking of leaving, but yeah we came back to London [and] things eventually fizzled out with the manager with us being here and them there and I think we missed a great oppurtunity but who knows, maybe it just wasn’t meant to be.
In interviews both you and John stated that the Glitterati was one of those bands that if something could go wrong, it would go wrong. Yet at the same time, you seemed to have enough luck or momentum to make quite an impact – having chart success with your singles before being snapped up by Atlantic, getting a TV slot before you had released an album, and touring with some big bands like the Wildhearts. You even opened in Wembley. Was the bad luck down to any turmoil within the band, or did it just feel like fate was against you?
We always felt like we had bad luck at the time, I’m sure a lot of bands do, it’s why most bands can all see Spinal Tap in themselves.We always had the ability to laugh at it, and when i look back we had a lot of good luck too.
The main thing was probably not luck but timing, we moved to London at the right time, the industry were looking for a band like us, [so were] the labels and the press. This allowed us to sign a huge deal and live out all our dreams, it was the best time of my life and I’m grateful for that.
We also had bad timing, there was a year between us signing with Atlantic and releasing our album; a lot had changed in 12 months, there was a backlash against The Darkness in the music press, and us being a rock band on the same label we were kind of lumped in with all that, and also a lot changed at Atlantic.
It had been a year since they signed us and a LOT can change at a major label in a year. By the time the album was released a lot of our supporters at the label had left and we were always fighting an uphill battle there once the album came out. The same person who sat us down a year earlier and told us we should sign with them because they were a label who were interested in longevity and great albums and not just having hit singles blah blah blah told us they were going to get rid of us if our next single, which was only our third for them, didn’t go top 10 in the charts, and that was the day we set off on a 35-date headline tour – our biggest yet – so that was a tough time. Great way to run a label, sign a band for a huge amount of money, have no idea what to do with them once they’ve signed and give them 3 singles to have a top 10 hit, you really couldn’t make some of it up but that’s pretty much the standard blueprint for major labels, or it was then, now you don’t even get the fun part of blowing loads of money but the rest is still pretty much the same.
I think for fans the band’s break-up felt as sudden as how quickly you emerged – you released ‘Fight Fight Fight’ as a single, released the album, and were waiting to embark on a headline tour but instead broke up. On the New Kings of Rock N Roll show you stated that a lot of bands don’t give it the time to get successful and break up too early. Do you felt that the band broke up prematurely, that it would have been easier to continue with the Glitterati than start from the ground up again in a new band, or was it the only real option?
We really tried to make it work,we tried everything,we had such high hopes for the second album. We funded the recording, got a great producer in Matt Hyde, we shopped it round labels ourselves, at times it was soul destroying and there were probably times where we all thought about splitting up, but we managed to hold it together and eventually signed to Demolition, who released the second album.
The plan was lots of touring to promote the album, both here and Europe where we had never really toured, but the touring never happened, through no fault of ours. We had a co-headline tour that fell through at the last minute as the other band’s agent felt they should headline all the shows. I won’t mention the other band but to be honest it was laughable that either they or their agent suggested that, so the day we were going to announce it we were off that tour, we were told not to worry as we were guaranteed the european tour with the New York Dolls. That fell through too.
So we were now left with an album that had been out months and nothing had been done to promote it, if we had good management at this point we could maybe have salvaged it but doing it ourselves and just coming up against brick walls everywhere eventually just ground us down and I don’t think any of us had the energy to fight for it anymore. John actually left the band a month or two before we split, we thought about finding a new guitarist but I think we all knew the band had naturally come to an end. It’s sad to me even now talking about it as it was a great band that should have done more, but I’ve nothing but amazing memories, I got to be in a band with my best mates and we were my favourite band, I had the time of my life, and everything has to end some time.
Were the hard times with the labels what inspired songs like Overnight Superstar?
Yes it is, a lot of that second album was about things that happened with the label and stuff. Lyrically it’s an angrier record than the first, the first album is about 5 mates having the time of their lives and being slightly naive and wide eyed to everything that was happening, and the second is more about dealing with the aftermath of that, trying to keep things together – friendships, relationships, the band – and basically wondering what the fuck happened to us and what do we do next. Regardless of the fact we didn’t get to give it anywhere near the promotion it deserved I’m still proud we at least got that second album out there, as the two albums pretty much tell our whole story, the good times and the bad. It nearly killed us getting it out there but at least we managed it in the end.
Two of the original members quit before the second album was recorded, how did that affect things?
When Nic and Jamie left the band it was really tough, it sounds silly and probably is but it really is like someone walking out of a marriage as it’s such a big part of everyones life. When they left it was tough,we had begun talking with Matt Hyde about producing the album and stuff, and [were] just about to set off on a UK headline tour so we were all pretty optimistic, so it was a bit out of the blue.
We were rehearsing for tour and Jamie rang and told us he was leaving the band, but would do the rehearsals and tour, which was actually pretty brave as he could have just left us in the lurch. The rehearsals were a bit tense but we got through that tour the best we could, I think the tour went pretty well, we were all laughing and joking about him ditching us and stuff, definitely gallows humour. It was really sad on that last gig in the dressing room, we had all been through so much, we were like a gang and this was the first chink in the armour. I’m pretty sure we all tried to be super manly about it and make out like it wasn’t a big deal and stuff but it was a sad time.
We were all determined to carry on, but Nic had been pretty quiet the whole tour, I just thought it was because him and Jamie were the closest so he didn’t really want to talk about replacements or anything, but I remember near the end of the tour getting the feeling Nic was about to jump ship too. I dont know if he and Jamie had both talked about leaving and decided between them not to both do it at the same time for the good of the tour, but a day or so after the tour ended Nic called me and said he was leaving too, so we were down to a 3 piece.
It was a tough time,when you are so into something, and it’s your life you can’t understand why someone else feels differently and would walk away from it, but they had their reasons and did what was best for them, it just wasn’t their whole life anymore and they wanted to do something else.
We went on to get Baz in and Gaff as replacements and getting new guys in definitely lifted the morale. They hadn’t been through the shit we had and had enthusiasm and excitement for everything, which was just what we needed at that point. Making the second album was so much fun, getting a second record deal was exciting too and we had some great times with the new line up, it’s just a shame we couldn’t have had a few more.
All of us have moved on to different things now but we will always be connected through the amazing times we had. It was a great time in all our lives, and I’m glad I got to share it with my mates because at the end of the day we were just mates doing the things we had always dreamed of doing.
I gather that you’re putting together, or have put together, a new band now. How’s that progressing, and is it anyone people may have heard of?
Yes i have, I’ve been working on it for a while, for a lot of reasons it’s taken longer than I imagined, but it’s really starting to come together now. I’m really enjoying it and I’m excited for people to hear it. I’m taking my time, I don’t feel under any pressure, I just want to make the kind of music I want to hear and hope other people like it too.
What can we expect from the new band sound-wise, and when can we expect to see you playing on the live circuit again?
It won’t sound like the Glitterati, I just don’t see the point, and I wouldn’t want to be in another band with a similair style as we may as well have just carried on. I’ve had the chance to join a few and it would have been the easier and maybe the more accepted thing to do, but I need to do something different,and right now if I was playing that kind of music my heart wouldn’t be in it, so like I said I’m just doing what i love first and foremost and hope lots of other people like it. If they don’t, I’ll live, ha ha!
If I’m honest, as much as I still love bands like GNR and New York Dolls it’s not something I really listen to much these days. Don’t get me wrong, I love those bands but it doesn’t influence my songwriting anymore. I’ve always been really into 50s rock n roll and I’m really into a lot of old blues stuff. The new band has elements of that, it’s kind of dirty, bluesy, vintagey rock n roll.
When the Glitterati disbanded, did you ever feel like throwing in the towel on music and trying something else, or is this all you’re compelled to do?
No I’ll never stop making music. I didn’t want to be in a band for a while after the Glitterati, that’s why it’s taken so long. I started the new thing on my own, I was just writing songs [and] I didn’t know if it would be a band. I thought I’d just get mates who are musicians to help me record whenever I needed to but as it went along I started wanting a more permanent thing again, I missed the laughs you have as a band and I missed having people to make music with.
Going off-topic, you’ve said before that you think Appetite for Destruction is the best rock album ever made – and millions would agree with you. The hot topic right now is Guns N’ Roses being inducted into the Rock N Roll Hall of Fame next month, as a fan what’s your opinion on that, and do you think they will, or should, put their differences aside to play on the night?
I still think it is, I have a lot of people who I know who are quite close to the band members so I hear a lot of different stories and different opinions. My personal opinion is I’d love to see them put their differences aside, it would be amazing for the fans, [but] I’m not sure if they ever will. The bad feeling between Axl and Slash obviously runs deep, it would take a lot of egos being left at the door and there are some massive massive egos involved. I hope it happens one day, but I think time’s almost up on them doing it and it still being cool – I dont want to see them up there at 70………….actually I probably would still want to see it, but I dont want it to be a train wreck.